The Influence of Body Position on the Blood Flow of Parenchymatous Organs: I. Liver
Human Physiology, Vol. 24. № 4. 1998, pp. 475-48O. Translated from Fiziologiya Cheloveka. Vol. 24. №4. 1998. pp. 101-107. Original Russian Text Copyright © 1998 by Minvaleev, Kuznetsov, Nozdrachev.
The Influence of Body Position on the Blood Flow of Parenchymatous Organs: 1. Liver
R. S. Minvaleev, A. A. Kuznetsov, A. D. Nozdrachev
Received February 4,1998
Abstract — The study included 30 subjects who were subjected to ultrasound dopplerography of arterial inflow and venous outflow in different organs while assuming positions from hatha yoga practice. To reveal the hemo-dynamic equivalents of the possible autonomic effect of yoga positions, we studied the intrahepatic blood flow in the "plough" position ("halasana"). Pulse blood flow in the right branch of the proper hepatic artery in the halasana position was reduced, while minute blood flow remained the same as prior to exercise activity. Portal vein flow also remained the same. Thus, minute blood filling of the liver during this test did not change. However, venous outflow at the moment of right-atrial systole underwent considerable changes. Prior to the beginning of exercise, 21 test subjects showed partial return of blood to the liver, and, during exercise, the mean value of linear blood flow in this phase was negative; i.e., it acquired a monophase character. Thus, the subjects who most adequately performed this exercise showed a blood flow "portalization" effect in the hepatic veins. A therapeutic effect of halasana was recorded, in which the initially changed monophase hepatic outflow (in a patient with hepatitis in her case history) was restored to the triphase one immediately after exercising.
Our physiological investigations of the hemodynamic features in various body positions [1, 2] were aimed at studying intraorgan blood flow in the parenchymatous organs. We assumed that the functional state of an organ is specified by the character of its blood supply. Since the liver is the largest digestive gland and the body’s biochemical laboratory, we decided to choose it for studying blood inflow to and outflow from this organ during the yoga exercise known as the halasana or plough position (Fig. 1).

Fig. 1. Plough position known in yoga exercises as halasana.
METHODS
The study involved 33 subjects (nine males and 24 females) between the ages of 18 and 55 years old who were taught to perform the plough position. Arterial inflow to the liver was studied in the first stage, and venous outflow was studied in the second stage.
Hepatic blood flow was studied with the help of echo-chambers [HITACHI EUB-525 (Japan) and KONTRON Sigma-44 (France)] and sensors for abdominal studies with a scanning frequency of 3.5 mHz. Blood flow in the right hepatic vein, the right branch of the proper hepatic artery, and the right branch of the hepatic portal vein was studied noninvasively by the method of pulse-wave dopplerography with the lateral approach from the right abdominal side or through the intercostal space on the right anterior line. Location of the arterial branch of the proper hepatic artery was the most difficult. It was visualized near the right branch of the hepatic portal vein in the regimen of color Doppler mapping. The right approach was used as the only possible one during the plough position exercise (Fig. 2). The same depth of the controlled volume of the sounding beam was used in each patient to record blood flow prior to yoga activity in a horizontal position on the back, during activity, and then immediately after activity in the same zone of the studied vessel. This condition was observed in order to obtain comparable blood flow parameters. Hepatic arterial flow was determined in 11 subjects. The comparable parameters included the maximal (Vmax) flow velocity in cm/s, the medium (Vmed) flow velocity in cm/s, the flow velocity integral (FVI) per one cardiac cycle and per one minute (flow) in cm, and also indexes showing muscular activity of the arterial wall: the pulse (PI) and resistance (RI) indexes in arbitrary units. Hepatic vein flow was studied in 22 subjects; their vein diameter, maximal portal flow Vp (сm/s), hepatic vein flow [peak velocities (in cm/s)] systole (Vs), end systole (Ves), diastole (Vd) and atrial-systole (Va) were determined. Heart rate (HR) per minute was also recorded. Hepatic vein flow was determined during breath holding [3,4]. Statistical processing was performed with the help of the packet of applied programs STATGRAFICS; the significance of differences was determined according to Student’s t-test for coupled samples.
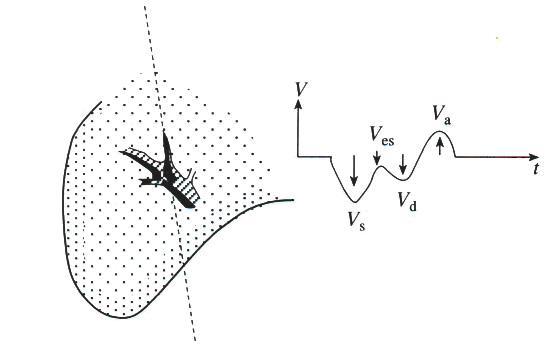
Fig. 2. Profile of blood flow velocity in the hepatic vein in healthy subjects.
RESULTS
The results of arterial flowmetry in the right hepatic lobe prior to, during, and after performing the plough position are presented in Table 1. An analysis of these data shows that FVI was the only parameter that changed from the initial level (0.5±0.2 cmprior to the position, 0.17±0.02 cm, pFlow=FVI · HR) remained the same (15.0±1.3 and 13.1±1.4 cm, pPIand RI and Vmax and Vmed remained the same. None of the measured parameters in the test subjects were different from the initial values after exercising. The parameters of venous in- and outflow in the hepatic right lobe are given in Table 2.
Table 1. Dynamics of parameters of arterial hepatic inflow in the plough position or halasana (n=11).
|
Parameters |
Initial X±m |
Position |
After exercise |
||
|
X±m |
p |
X±m |
p |
||
|
Vmax, cm/s |
0.41±0.04 |
0.39±0.05 |
nd |
0.38±0.04 |
nd |
|
Vmed, cm/s |
0.25±0.02 |
0.21±0.02 |
nd |
0.23±0.03 |
nd |
|
FVI, cm |
0.25±0.02 |
0.17±0.02 |
* |
0.23±0.03 |
nd |
|
Flow, cm |
15.00±1.30 |
13.10±1.4 |
nd |
13.60±1.6 |
nd |
|
PI, arb. units |
1.12±0.05 |
1.33±0.17 |
nd |
1.26±0.16 |
nd |
|
RI, arb. units |
0.68±0.02 |
0.70±0.03 |
nd |
0.70±0.03 |
nd |
|
HR, stroke/min |
60.6±3.5 |
78.4±4.8 |
** |
60.6±4.0 |
nd |
Note: Vmax, maximal flow velocity; Vmed, medium flow velocity; FVI, flow velocity integral per one cardiac cycle; Flow, flow velocity integral per 1 min; Pl, pulse index; Rl, resistance index; HR, heart rate. Significance of diferences: * p
Table 2. Dynamics of hepatic vein flow parameters in the plough position or halasana (n=21, general group)
|
Parameters |
Initial X±m |
Position |
After exercise |
||
|
X±m |
p |
X±m |
p |
||
|
Dpv, mm |
7.7±0.4 |
7.3±0.4 |
nd |
7.5±0.3 |
nd |
|
Vp ,cm/s |
25.0±1.4 |
26.5±1.8 |
nd |
23.0±1.6 |
nd |
|
Dhv , mm |
7.0±0.4 |
5.8±0.4 |
nd |
6.9±0.3 |
nd |
|
Vs , cm/s |
-32.7±2.3 |
-27.4±2.6 |
nd |
-32.1±2.2 |
nd |
|
Ves , cm/s |
-6.6±2.3 |
-4.3±3.0 |
nd |
|
|
|
Vd , cm/s |
-17.5±1.6 |
-16.6±1.8 |
nd |
|
|
|
Va , cm/s |
12.0±1.1 |
-1.6±4.2 |
** |
15.0±1.5 |
nd |
|
HR, stroke/min |
69.7±3.2 |
90.2±4.7 |
*** |
74.2±2.9 |
nd |
Note: Dpv, portal vein diameter; Dhv, hepatic vein diameter; Vp, maximal portal flow; Vs peak flow velocity in the hepatic vein during systole; Ves, peak flow velocity in the hepatic vein at the end of systole; Vd, peak flow velocity in the hepatic vein during diastole: Va, peak flow velocity in the hepatic vein during atrial systole; HR, heart rate. The absence of data on Ves and Vd during exercise is explained by the sharp change in the flow character at this moment in most test subjects. Significance of differences: * p < 0.05: ** p < 0.01; nd, no significant differences.
During exercise, the diameter of the right branch of the hepatic portal vein (7.7±0.4 mm and 7.3±0.4 mm, p>0.05), and the blood flow recorded in it did not change (V in the initial state was 25.0±1.4 cm/s; during the plough position, it was 26.5±1.8 cm/s, p>0.05). The branch of the right hepatic vein also had no changes in its diameter (6.8±0.4 and 5.8±0.5 mm, p>0.05). Blood flow during systole was also stable (32.7±2.3 cm/s in the initial state and 27.4±2.6 cm/s, during exercise, p>0.05). Since most of the test subjects showed sharp qualitative changes in hepatic vein outflow, blood flow could not be recorded at the end of right-ventricular systole or at the beginning of diastole during exercise. On the contrary, blood flow at the moment of right-atrial systole changed considerably. Prior to exercise, 21 test subjects had positive Va (-12.0±1.1 cm/s) for mean partial return of blood to the liver, while, during exercise, the mean value of linear flow in this phase was negative (-1.6+4.0 cm/s, pVa blood flow. In the first group, 9 of 21 subjects (summary data are given in Table 2) had monophase venous outflow with the disappearance of the phase pulsatory (waveform) character of its variations (Fig. 3). Eight subjects of the second group maintained the pulsatory character of outflow, but the return phase to the liver was absent during right-atrial contraction (Fig. 4). In the third group, blood flow in four subjects during exercise remained the same and was triphase.
Fig. 3. Development of nonpulsatory monophase hepatic vein outflow during halasana: on the left is the initial stale; on the right is during exercise.
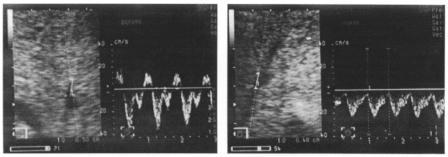
Fig. 4. Development of pulsatory two-phase hepatic vein outflow during halasana: on the left is the initial state: on the right is during exercise.
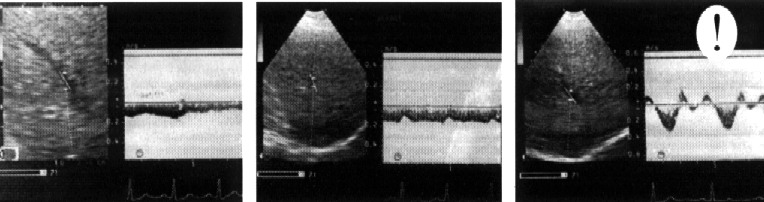
Fig. 5. Restoration of normal triphase hepatic vein outflow in a female patient with initially pathological monophase hepatic vein flow: on the left is the initial state; in the center is during exercise; and on the right is after exercise.
Separate estimates of the results of studying the subgroups with monophase (M) and pulsatory (P) hepatic outflow during the plough position (see Table 3) showed that, in the initial state, subjects with monophase outflow during exercise were different from eight other test subjects; i.e., they had lower inflow velocity in the portal vein Vp (21.0±2.0 and 27.7±1.3 cm/s, ps was higher in pulsatory outflow than in monophase outflow (-31.4±4.1 and -19.5±2.9 cm/s, pa flow (interrupted outflow was noted), the blood flow changed direction, on average, in both subgroups (pa: subgroup P, -11.9±4.2 cm/s and subgroup M, -9.6±1.0 cm/s, pM, 93.9±7.4 stroke/min and subgroup P, 95.2±8.3 stroke/min, p0.05 between groups). No changes were found in other parameters during exercise. Portal vein inflow after exercise was reduced in subjects with pulsatory venous flow to 21.2±1.4 cm/s (pM (-26.1±2.3 cm/s versus -35.5±3.8 cm/s, pP(18.5±2.2 cm/s versus 10.4±1.4, p
Table 3. Dynamics of parameters of hepatic vein circulation during the plough position: in subgroups with monophase (M, n=9) and pulsatory (P, n=8) outflow
|
Parameters |
Sub-group |
Initial |
During exercise |
After posture |
|||
|
X±m |
p |
X±m |
p |
X±m |
p |
||
|
Dpv , mm |
M |
7.5±0.7 |
nd |
7.2±0.7 |
nd |
7.7 ±0.5 |
nd |
|
P |
7.4±0.7 |
7.0±0.6 |
nd/nd |
6.8±0.5 |
nd/nd |
|
|
|
Vp , cm/s |
M |
21.0±2.0 |
* |
24.9±3.6 |
nd |
24.6±3.2 |
nd |
|
P |
27.7±1.3 |
28.0±2.3 |
nd/nd |
21.2±1.4 |
**/nd |
|
|
|
Dhv mm |
M |
6.1±0.5 |
nd |
5.6±0.6 |
nd |
6.5±0.4 |
nd |
|
P |
7.5±0.9 |
5.1±0.9 |
nd/nd |
6.9±0.4 |
nd/nd |
|
|
|
Vs , cm/s |
M |
-25.9±2.0 |
* |
-19.5±2.9 |
nd |
-26.l±2.3 |
nd |
|
P |
-36.5±3.6 |
-31.4±4.1 |
nd/* |
-35.5±3.8 |
nd/* |
|
|
|
Ves , cm/s |
M |
-1 1.4 ±3.3 |
nd |
- |
- |
-11.3±3.7 |
nd |
|
P |
-4.0 ±3.3 |
- |
-/- |
-2.8 ± 4.6 |
nd/nd |
|
|
|
Vd , cm/s |
M |
-18.0±2.7 |
nd |
- |
- |
-16.2±2.6 |
nd |
|
P |
-18.0±2.5 |
- |
-/- |
-17.8±3.5 |
nd/nd |
|
|
|
Va, cm/s |
M |
9.9±1.4 |
nd |
-9.6 ±1.0 |
** |
10.4±1.4 |
nd |
|
P |
12.8±1.5 |
-11.9±4.2 |
***/nd |
18.5±2.2 |
*/** |
|
|
|
HR, stroke/min |
M |
71.7±2.9 |
nd |
93.9±7.4 |
** |
74.3±2.9 |
nd |
|
P |
68.8±6.8 |
95.2±8.3 |
*/nd |
80.8±5.2 |
nd/nd |
|
|
Note: In subgroup P, the significance of differences (p) in the nominator is relative to the initial state: in the denominator, in a given moment between groups.
DISCUSSION
It has been established that, in the event of poor blood circulation, when the left-ventricular stroke volume drops, both linear and volume flow velocity are reduced in the general hepatic artery [9]. In our case, each cardiac cycle was followed by a significant decrease in arterial inflow in its largest (i.e., right) branch. We can state this with sufficient reliability proceeding from the analysis of blood flow in an arterial branch of small (about 1.5 mm) diameter. In this case, we suggest that the cross sections of these arteries had few variations in different test subjects and that the estimation of the velocity integral correlated sufficiently well with volume flow via the vessel during one cardiac contraction. The developing tachycardia ensured maintenance of minute arterial flow to the liver at the initial level. There were no changes in the parameters of muscular activity of the arterial wall (PI and Rl). The fact that no arterial spasms were observed in the plough position indicates that a decrease in FVI is caused by changes in central hemodynamics. At the hepatic level, these changes were compensated for by cardiac contraction acceleration. There were no changes in hepatic vein inflow in the general group or in the subgroups during exercise. Considering the results of arterial flow analysis, it can be stated that hepatic minute blood filling is stable during the plough position. Differences in Vp were found during exercise depending on the type of hepatic vein outflow. Subjects with developing monophase outflow presented lower portal inflow in the initial state, and, during and after exercise, the differences leveled off. In this case, portal vein flow decreased in test subjects with pulsatory hepatic outflow after exercise. Polish scientists reported [10] that in healthy subjects there was a dependence between body mass and portal flow. In our case, no intergroup differences in body mass were found. Thus, the subgroups of our test subjects had certain differences in portal flow. Differences in hepatic outflow were more pronounced. During exercise, subjects with pulsatory outflow showed higher outflow than the other subgroup during right-ventricular systole in all examination stages. It should be noted that the changes in hepatic vein blood flow discovered by us during exercise are well-known in clinical practice. Flat monophase hepatic outflow is often found in liver cirrhosis [5-7]. In hepatitis, all three patterns of hepatic outflow are observed: unchanged triphase, pulsatory without a blood phase during atrial systole, and monophase nonpulsatory flat flow [4, 5]
Note: Changes in hepatic vein outflow are affected by the development of direct intrahepatic anastomoses between branches of the portal and hepatic veins and multiple arterio-portal bypasses [11]. It is difficult to evaluate the action of these mechanisms in our case. since this is associated with situations leading to portal hypertension, which is manifested by widening of the portal vein and acceleration or slowing down of blood flow in it. We did not find changes in the diameter or linear velocity of blood inflow in the portal vein during the halasana position.
There was no clear correlation between manifestation of changes in hepatic outflow and the degree of hepatic parenchyma damage. On the contrary, it was found that all subjects having monophase hepatic outflow during exercise had sufficient experience in its performance and most of them were yoga specialists. Three out of four test subjects who showed no changes in hepatic outflow were beginners, and one subject simply could not master the position. He confessed that he never experienced the sensation of "heat" in the subcostal region, which had to be achieved during the halasana position. Moreover, some of the test subjects were able to enhance the feeling of liver contraction at the command of the instructor during exercise, which was followed by a change from pulsatory outflow to monophase outflow from the liver (Fig. 3). This circumstance and the technical features of the halasana position, when the exercise consists in a decrease in the volume of the abdominal cavity and mechanical pressure on the liver, lead us to the conclusion that pulsatory and monophase hepatic vein blood flows pass into one another as intrahepatic squeezing of the proper hepatic veins in the organ increases. The case when the initially changed monophase hepatic outflow became a common triphase outflow after performing the halasana position with a clear flow reversal phase to the liver during right-atrial systole is undoubtedly of clinical interest. Most of the test subjects assessed their state after exercise as a feeling of relaxation and comfort radiating from the liver, which gives grounds to hope that this exercise can be used for therapeutic purposes. Comparisons of the changes that we observed with the report on the dynamics of hepatic vein outflow during intrauterine development of humans are interesting. The authors [12] found an increase in the rate of formation of a flat wave of hepatic vein flow in a fetus as pregnancy developed. Proceeding from our results, we can suggest that the effect of a sharp decrease in the transmitral pressure in the hepatic veins occurs immediately after delivery. Then, the exercise discussed helps create conditions for increased squeezing of the hepatic veins during the short duration of this exercise (usually, not more than one minute) with the subsequent effect of sharp cessation of hepatic vein compression.
CONCLUSIONS
1. During the exercise known in yoga as the plough position, the minute blood filling of the liver through the hepatic artery and portal vein remains unchanged.
2. In the plough position most subjects show monophase nonpulsatory or pulsatory two-phase hepatic vein outflow instead of the usual triphase outflow with a partial return of blood to the liver.
3. The specific features of the initial hepatic portal and venous blood flow can predetermine the character of hepatic flow changes during the plough position exercise.
4. After the plough position exercise, the common triphase hepatic vein outflow is fully restored; a therapeutic effect of this exercise was recorded when the initially changed monophase hepatic outflow (in a female patient with hepatitis in her case history) became triphase immediately after exercise.
REFERENCES
1. Ebert D., Physiologische Aspekte des Yoga. Leipzig: Georg Thieme, 1988.
2. Minvaleev R.S., Kuznetsov A.A., Nozdrachev A.D., and Lavinskii.Yli.Kh., Left Ventricle Filling in Sirshasana and Sarvangasana Yogic Postures, Fiziol. Chel., 1996, vol. 22, №6, p. 27.
3. Beresten’ N.F., Two-Dimensional Pulse Dopplerography in Chronic Hepatitis, Sov. Med., 1991, no. 5, p. 24.
4. Minich L.L., Tani L.Y., Shaddy R.E. and Snider A.R., Doppler Systemic Venus Flow Patterns: Changes in Children with Mild/Moderate Pulmonic Stenosis, J. Am. Soc. Echocardiogr., 1996, vol. 9, №6, p. 814.
5. Arda K., Ofelli M., Calikoglu U. et al. Hepatic Vein Doppler Waveform Changes in Early Stage (Child-Pough A) Chronic Parenchymal Liver Disease, J. Clin. Ultrasound, 1997, vol. 25, №1, p. 15.
6. Gorka, W., al Mulla, A., al Sebael, M., et al., Qualitative Hepatic Venous Doppler Sonography Versus Portal Flowmetry in Predicting the Severity of Esophageal Varices in Hepatic C Cirrhosis, Am. J. Roentgenol., 1997, vol. 169, №2, p. 511.
7. Parra Blanco, J.A., Juanco Pedregal, C., and Silvan Delgado, M., Changed Hepatic Vein Flow in Patients with Cirrhosis: A Doppler Study of Hepatic Veins in Patients with Cirrhosis, Rev. Esp. Enferm. Dig., 1995, vol. 87, №9, p. 621.
8. Uemo, S., Tanabe, G., Sueyoshi, K., et al., Hepatic Hemodynamics in a Patient with Nodular Regenerative Hyperplasia, Am. J. Gastroenterol., 1996, vol. 91, №5, p. 1012.
9. Zadionchenko, VS. and Tirnofeeva, N.Yu., State of Arterial and Portal Blood Flow in Patients with Poor Blood Circulation, Vtoroi kongress Assotsiatsii spetsialistov ul’trazvukovoi diagnostiki v meditsine (Second Congress of the Association of Specialists in Ultrasound Diagnosis in Medicine), Moscow, 1995, p. 51.
10. Kalina, Z., Scieszka, J., and Maslankiewicz, A., Doppler Measurement of Blood Flow in the Portal System of Healthy Volunteers, Pol. Arch. Med. Wewn., 1989, vol. 82, №№4-6, p. 168.
11. Kuntsevich, G.I., Belolapotko, E.A., and Sidorenko, G.V, Assessment of Portal Circulation in Patients with Liver Cirrhosis by the Data of Duplex Scanning, Vizualizatsiya v Klinike, 1994, №5, p. 33.
12. Roobottom, S.A., Hunter, J.D., Weston, M.J., and Dubbins, PA., Hepatic Venous Doppler Waveforms: Changes in Pregnancy, J. Clin. Ultrasound, 1995, vol. 23, №8, p. 47.